Myocardial infarction
From Wikipedia, the free encyclopedia
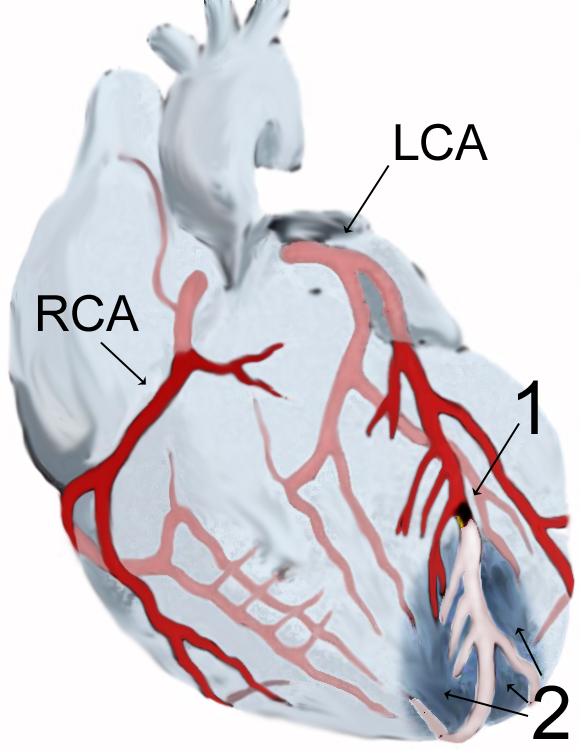
Diagram of a myocardial infarction (2) of the tip of the anterior wall of the heart (an apical infarct) after occlusion (1) of a branch of the left coronary artery (LCA, right coronary artery = RCA).
Acute myocardial infarction (AMI or MI), more commonly known as a heart attack, is a medical condition that occurs when the blood supply to a part of the heart is interrupted, most commonly due to rupture of a vulnerable plaque.
The resulting ischemia or oxygen shortage, if left untreated for a sufficient peroid, can cause damage and/or death of heart tissue. It is a medical emergency, and the leading cause of death for both men and women all over the world.[1] Important risk factors are a history of vascular disease such as atherosclerotic coronary heart disease and/or angina, a previous heart attack or stroke, any previous episodes of abnormal heart rhythms or syncope, older age—especially men over 40 and women over 50, smoking, excessive alcohol consumption, the abuse of certain drugs, high triglyceride levels, high LDL (low-density lipoprotein, "bad cholesterol") and low HDL (high density lipoprotein, "good cholesterol"), diabetes, high blood pressure, obesity, and chronic high stress levels. Chronic kidney disease[2] and a history of heart failure[3] are also significant risk factors which may indicate a hightend disposition towards suffering a MI.
The term myocardial infarction is derived from myocardium (the heart muscle) and infarction (tissue death due to oxygen starvation). The phrase "heart attack" is sometimes used incorrectly to describe sudden cardiac death, which may or may not be the result of acute myocardial infarction. A heart attack is different from, but can be the cause of cardiac arrest, which is the stopping of the heartbeat, and cardiac arrhythmia, an abnormal heartbeat. It is also distinct from heart failure, in which the pumping action of the heart is impaired; severe myocardial infarction may lead to heart failure, but not necessarily.
Classical symptoms of acute myocardial infarction include chest pain (typically radiating to the left arm or left side of the neck), shortness of breath, nausea, vomiting, palpitations, sweating, and anxiety (often described as a sense of impending doom). Patients frequently feel suddenly ill. Women often experience different symptoms from men. The most common symptoms of MI in women include shortness of breath, weakness, and fatigue. Approximately one fourth of all myocardial infarctions are silent, without chest pain or other symptoms. A history of diabetes should heighten the index of suspicion, particularly if the patient has diabetic neuropathy (diabetes-related nerve damage).
Immediate treatment for suspected acute myocardial infarction includes oxygen, aspirin, and sublingual glyceryl trinitrate (colloquially referred to as nitroglycerin and abbreviated as NTG). Pain relief is also often given, classically morphine sulfate.[4]
The patient will receive a number of diagnostic tests, such as an electrocardiogram (ECG, EKG), a chest X-ray and blood tests to detect elevations in the creatine kinase-MB (CK-MB) fraction or in troponin I (TnI) or troponin T (TnT) levels (these are chemical markers specific to the myocardium and are often referred to as cardiac markers). on the basis of the ECG, a distinction is made between ST elevation MI (STEMI) or non-ST elevation MI (NSTEMI). Most cases of STEMI are treated with thrombolysis or if possible with percutaneous coronary intervention (PCI, angioplasty and stent insertion), provided the hospital has facilities for coronary angiography. NSTEMI is managed with medication, although PCI is often performed during hospital admission. In patients who have multiple blockages and who are relatively stable, or in a few extraordinary emergency cases, bypass surgery of the blocked coronary artery performed by a cardiothoracic surgeon is an option. once admitted to hospital, the patient is observed on a coronary care unit, as the incidence of sustained ventricular tachycardia or ventricular fibrillation in the case of MI is high. In cases where the patient is unstable, more intensive nursing care may be warranted.
'연구하는 인생 > 西醫學 Medicine' 카테고리의 다른 글
| 생활습관병(성인병)과 가족력 (0) | 2011.01.10 |
|---|---|
| Stroke (Cerebrovascular Infarction) (0) | 2011.01.07 |
| What Are the Signs and Symptoms of Atrial Fibrillation? (0) | 2011.01.05 |
| **** 건강샘 질병정보 Health A to Z **** (0) | 2011.01.05 |
| 腦梗塞 stroke (0) | 2011.01.05 |